Nutrition Diagnosis
Nutrition Diagnosis
Bookmark this page for easy reference in the future: Make sure to scroll down to see all the examples of P’s, E’s, and S’s that might align with your client cases.
Just getting started with supervision? You’ll need to write a successful PES statement to meet this competency for your Competency Check #1 meeting , please choose one of the cases listed below, scroll down to see the posisble P’s, E’s and S’s you might want to use to craft your sentence, and work up a PES statement. You can also use this same client to fill out your sample chart note for competency 10. To demonstrate the competency, be prepared to share your chart note during your Competency Check #1 meeting.
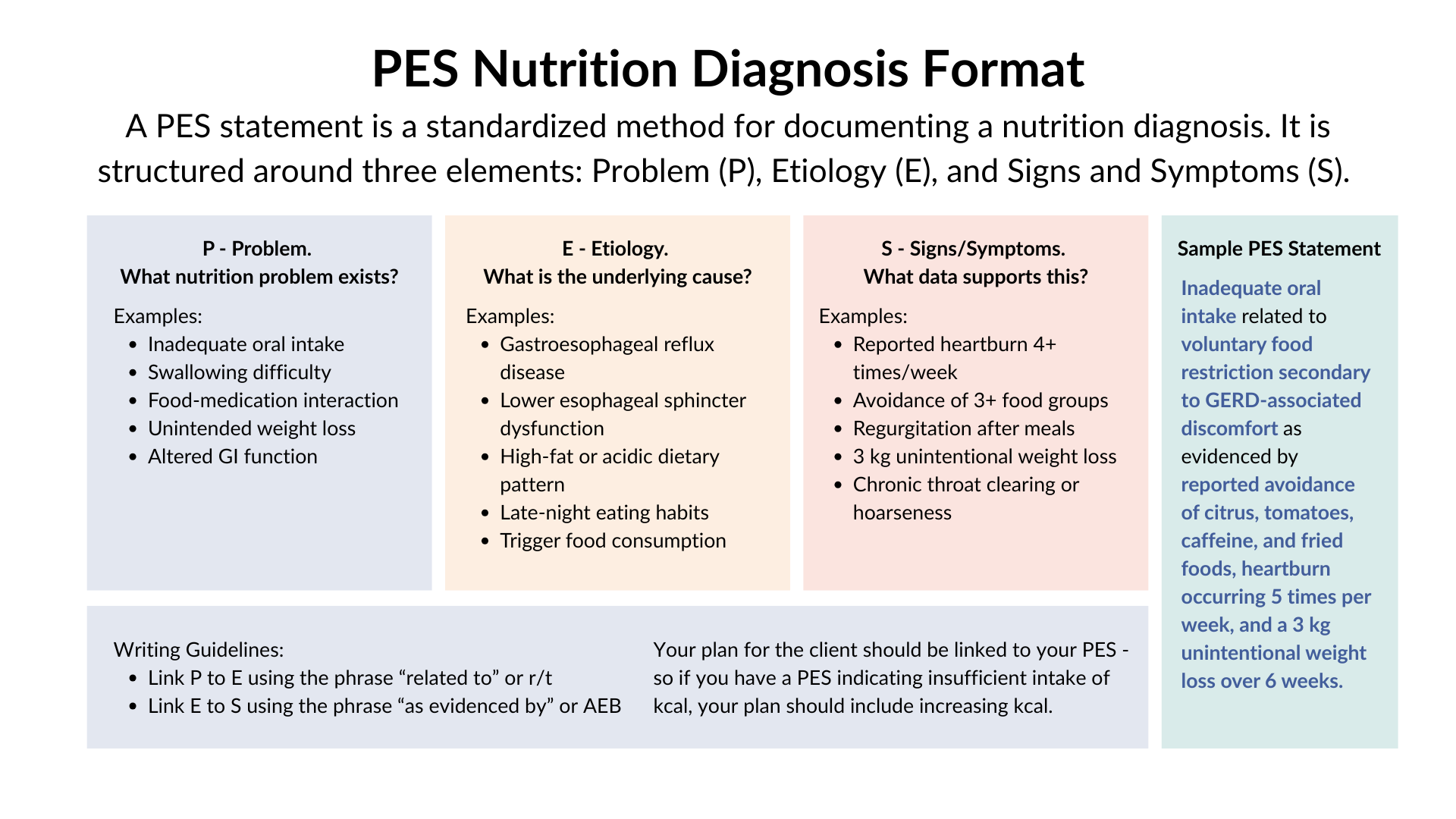
To get things started, here’s an example of how to write a PES for a Case:
Case Description: A 32-year-old Asian female; reports recent diagnosis of pre-diabetes with an HbA1c of 6.0, fasting insulin of 18, and fasting blood glucose of 102. Client reports decided to become vegetarian 1 year ago due to ethical concerns and diet changed from eating lots of seafood, chicken and pork with veggies and rice to the last 8 months eating mostly packaged vegan proteins (frozen veggie burgers, veggie sausages), with rice, some vegetables and occasional eggs. Ct has family hisotry of T2DM, and dementia. Ct is experiencing fatigue and increase in thirst.
PES: Nutrition related knowledge deficit r/t (related to) nutritional needs when shifting to vegetarian diet AEB (as evidenced by) dx pre-diabetes, HbA1c of 6.0, fasting insulin of 18, and fasting blood glucose of 102, diet record showing reliance on processed plant proteins, inadequate total protein intake, inadequate B-12 and o-3 intake.
OR here is another option for the same client (sometimes you might have more than one PES for a client case):
PES: Increased need for protein, fiber, B-6, Mg, O-3s r/t recent shift to vegetarian diet, family hx T2DM, recent dx of pre-diabetes AEB HbA1c of 6.0, fasting insulin of 18, and fasting blood glucose of 102, diet record.
Pick one of the below cases to write your own PES, and scroll down for our cheat sheet:
Case Description
A 57-year-old Caucasian male; reports high levels of stress at work. Hates vegetables, is a "meat and potato guy". Consumes a 6 pack of beer per night to "wind-down". Does not see a therapist; reports they did not talk about mental health growing up. Labs show low serum B12, low serum folate, and high MCV.
A 62-year-old Hispanic male. reports frequent urination, excessive thirst, and weight loss. Skips breakfast, usually has a sandwich for lunch, and animal protein, starch, and one veggie for dinner. Drinks multiple cups of coffee during the day, and has to nap around 3 pm every day. Unable to exercise due to arthritis pain in knees.
Common Nutrition “Problems”
Intake:
Inadequate energy intake
Excessive energy intake
Inadequate fluid intake
Excessive fluid intake
Excessive alcohol intake
Increased nutrient needs:
Decreased nutrient needs:
Inadequate fat intake
Excessive fat intake
Inappropriate intake of fats
Inadequate protein intake
Excessive protein intake
Inadequate carb. intake
Excessive carb. intake
Inappropriate intake of carb.
Inadequate fiber intake
Excessive fiber intake
Inadequate vitamin/mineral intake:
Excessive vitamin/mineral intake:
Clinical:
Swallowing difficulty
Chewing difficulty
Altered GI function
Impaired nutrient utilization:
Food/medication interaction:
Underweight
Involuntary weight loss
Overweight
Involuntary weight gain
Inadequate milk production
Breastfeeding difficulty
Behavioral:
Food/nutrition knowledge deficit:
Harmful beliefs/attitudes re: food:
Not ready for diet/lifestyle change:
Disordered eating pattern
Undesirable food choices
Physical inactivity
Excessive exercise
Inability to prepare foods
Lack of access to food
Inability or lack of desire to manage self-care
Common Nutrition “Etiology”
Antecedent- Genetic SNPs
Antecedent- Family history of XYZ
Antecedent- Childhood exposure to environmental/cultural/social/medical/nutrition component
Antecedent - Placed on diet in childhood
Antecedent - ACES
Antecedent - Experienced family members discussing dieting/preoccupation with body image in childhood
Antecedent - Experienced family members with chronic illness in childhood
Trigger- Having had experienced Injury
Trigger- Having had experienced Food poisoning
Trigger- First diet at age XYZ
Trigger/Mediator- Exposure to Trauma
Trigger/Mediator- Exposure to Family/social dynamics
Trigger/Mediator- Exposure to Stress- health, family, work…
Mediator- Experiencing Knowledge deficit regarding nutrition, physical activity and/or health condition
Mediator- Experiencing Accessibility Barrier to food/medical services/exercise
Mediator- Experiencing Diagnoses (depending on “P,” diagnoses may be in “S”)
Mediator- Exposure to Medications- nutrient depletions, interactions, side effects
Mediator- Desire for thinness/focus on body ideal
Common Nutrition “Signs & Symptoms”
Symptoms:
Constipation
Diarrhea
Acid Reflux
Gas
Bloating
Bowel urgency
Straining with Bowel Movement
Brain fog
Fatigue
Difficulty concentrating
Anxiety
Low mood
Painful periods
Bloating during/before menstrual cycle
And so many more…
NFPE Findings:
Dry scalp/skin
Brittle nails, white spots on nails…
Easy bruising
Hyperkeratosis pilaris
Rashes
Stomatitis
Food Record Findings
Diagnoses (depending on “P”, diagnoses may also be in “E”)
Lab Findings
Elevated or low lab work- list specifically (ie. HbA1c 7.4-H, LDL 289-H, 25-OH-D 7-L…)
Test findings that are not WNL- list specifically (ie. elevated Methanobrevibacter smithii, polyps found during colonoscopy…)
Blood Pressure (H or L)